Future of Bridges | Florida bridge collapse has
some hard lessons
BY MARK HANSFORD - 16 DEC, 2019
A litany of failures ultimately combined to
cause the collapse of the Florida International
University (FIU) Bridge onto a live highway,
according to the official investigation into the
accident.
Key companies and organizations involved in the
project were criticized in the final report into
the collapse published by the US National
Transportation Safety Board (NTSB) (New Civil
Engineer last month).
Calculation errors
It concludes that design calculation errors made
by Figg Bridge Engineers were ultimately to
blame.
But failures by the independent design checker,
client, contractor and on-site construction
supervisor also contributed to the disaster,
which killed six people (see box). All had the
chance to act when serious cracks appeared in
the structure in the two days before the
collapse, but none did.
So this month we ask: what can we learn from
this failure?
Tony Gee & Partners group director of structures
Akram Malik, has spent 20 years examining why
structures collapse – particularly as a tool for
learning. So who better for New Civil Engineer
to ask to review the FIU collapse?
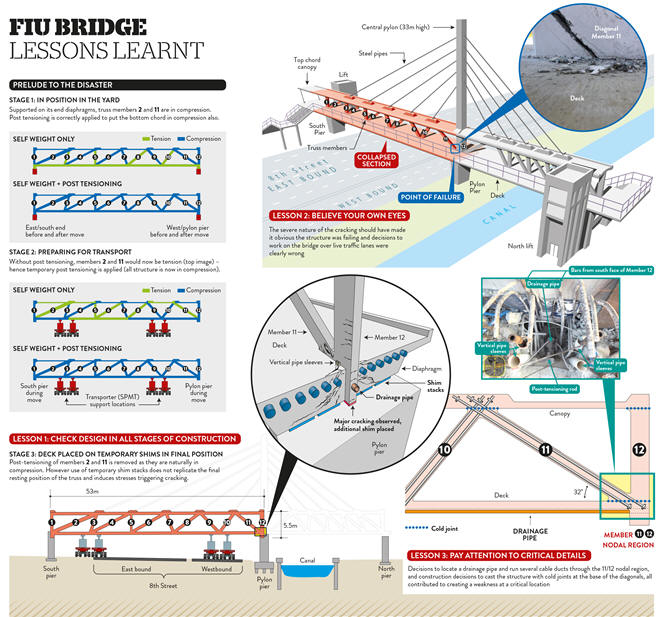
The structure included a 53m long prefabricated
main span made up of a 5.5m deep concrete truss
of 12 diagonal members. The truss supported the
10m wide deck and a 5m wide canopy running along
its length. The main span connected to a side
span around a central pier onto which a 33m tall
central pylon was to be built. This was an
architectural feature with 10 diagonal steel
“pipes” hanging from it to provide additional
stiffness but no other structural function.
It was at the connection between the two spans
and the pier – known as 11/12 nodal region –
that the failure occurred.
The client for the bridge was Florida
International University. It hired MCM as design
and build contractor, and MCM hired Figg as
designer and to serve as engineer of record.
Figg then contracted consultant Louis Berger to
conduct the required independent peer review of
the structural design. FIU also hired Bolton
Perez as construction engineering and inspection
contractor to monitor and inspect the bridge as
it was constructed. Florida Department for
Transportation (FDOT) is the highway authority
responsible for SW 8th Street, the road onto
which the bridge collapsed.
Independent checker role
Malik believes there are key lessons to be
learned, the clearest concerning the role of the
independent checker.
“Independent checking when required should
include every critical stage of construction,”
he states.
“Here, we’ve got Louis Berger who was engaged by
Figg, and Figg only asked it to look at the
final design, not the interim construction
stages – and both failed to see that the
intermediate construction stages were actually
critical in the failure”.
At face value the independent peer review
process was good. The structure was deemed a
“category 2” structure, for which the required
checks are similar to the UK Highways England’s
“category 3” process. “So a proper check was
required,” notes Malik, although he adds that
the exact requirements were unclear from
documents he has seen.

Computer image of Florida International
University Bridge
What is clear, from the NTSB’s report, is that
Louis Berger dropped its price from $110,000
(£84,000) under pressure from Figg whose budget
for this work was £46,500. Emails obtained by
investigators show Louis Berger warning Figg
that in seeking lower bids, FIU should be aware
that “a lesser fee may be associated with less
effort/value”.
More emails show that on contract award the
original scope of work remained unchanged, but
that Louis Berger had reduced the time it was
prepared to spend on checks from 10 weeks to
seven.
Peer reviewer requirements not met
Investigators also found that Louis Berger
failed to meet FDOT requirements for a peer
reviewer to employ at least three registered
professional engineers, each with a minimum of
five years’ experience in designing complex
concrete bridges.
Louis Berger performed the independent peer
review of Figg’s design using Adina, a finite
element analysis software program, in accordance
with FDOT standards. Post-collapse, Louis Berger
confirmed to NTSB investigators that it analyzed
the design as one structure in its completed
state. It only analyzed the design for the
completed structure and not for its various
construction phases.
“Doing construction sequence staging analysis
was not part of our scope. Doing such an
analysis requires much more time than what we
agreed about [with Figg],” it told
investigators.
The significance of failing to consider the
structure in its construction configurations
became clear when investigators began examining
the construction sequence, explains Malik.
The entire 53m long main span structure was
built off-site and then moved into its final
position on mobile transporters where it was set
on temporary shims.
Changing support system
Ahead of the move, the two end diagonals of the
truss were tensioned to ensure they remained in
compression while in transit (see diagram).
In the casting yard there was full contact
support across the deck and its two ends, yet
while resting on the pier the shims were placed
either side of the central truss – meaning there
was no direct support under the truss location.
This induced unexpected stresses and strains in
the structure which were exacerbated when the
end diagonal truss member was de-stressed after
it was positioned. This triggered the
significant cracking which should have given
warning that collapse was imminent. Such a
critical construction stage should have been
modelled by the checking engineer, Malik
concludes.
A second key lesson, says Malik, is the
old-adage of the devil being in the detail.
Investigators have overwhelmingly concluded that
the trigger for the collapse was punching shear
failure at the node where the end vertical and
diagonal truss members met. The NTSB has been
unequivocal in stating that Figg’s load and
capacity calculation errors at this key node
probably led to the failure. Post-collapse
calculations showed that the load demand on the
node was twice that designed.
Error went unnoticed
Louis Berger, as design checker, should have
noticed this error.
In a post-collapse interview, the Louis Berger
engineer who conducted the peer review told the
NTSB that the agreed budget did not stretch to
this level of analysis.
“In the beginning, I suggested to do this kind
of analysis, to analyze the connections,” he
said. “I’m talking about the nodes, or the
joints to analyze the connections. However, the
budget and time to do this actually was not
agreed upon with the designer.”
“Clearly in this case no-one looked carefully
enough at what was a really critical location,”
says Malik.
Malik points to a host of obvious deficiencies,
including decisions to locate a drainage pipe
and run several cable ducts through the critical
11/12 nodal region and construction decisions to
cast the structure with cold joints at the base
of the diagonals. He also questions the quality
of preparation of the construction joints.
“You have to look at the construction assurance
– was it wise to have the cold joint in such a
critical zone, that’s one question, and was it
prepared correctly? And we’ve got [on-site
supervisor] Bolton Perez Associates – did it do
its job? These are all questions that are a
little bit up in the air,” he says.
Retensioning to close cracks
One of the most alarming aspect of this collapse
was that the only action taken to stabilise the
structure – even when cracks up to 100mm deep
starting appearing – was to re-tension cables in
the end diagonal in the hope that this would
close the cracks.
Again, here there are clear lessons to learn,
says Malik. “In this case it appears that Figg
didn’t recognize that the structure was on its
way to collapsing.”
“It carried out calculations and those
calculations seemed to show that it was working
fine and that the cracks should not be
occurring.
“So it freely admitted that it didn’t understand
why the cracks were occurring, but on that basis
still decided to restress the bars to try and
arrest what was happening – even though it
didn’t understand it. This was poor decision
making,” he says.
Malik suggests that engineers should be educated
in the pre-collapse behaviour of structures. “Do
we need to include in our design processes an
additional question: ‘What are the ways in which
this structure could fail?’”
Malik’s final observation concerns the safety
management of the remedial action being taken –
restressing of the diagonal member above live
traffic.
“So… [site workers] were restressing the bars in
a critical member on a non-redundant structure
and were doing so over live traffic. Obviously
it was not a good decision in hindsight but even
in foresight it was not a good decision,” he
asserts.
And here he believes all parties should have
stepped in. But why didn’t they? “Are we
becoming too specialized?” he asks. Builders
build, designers design, supervisors supervise.
Is this preventing them from “exercising their
own independent professional judgement”?
Figg and MCM, Louis Berger and Bolton Perez have
been contacted for comment.
Investigators View: Bruce Landsberg - NTSB vice
chairman
A bridge-building disaster should be
incomprehensible in today’s technical world. We
have been building bridges in the United State
for over 200 years, and long before that in
other parts of the world. The science should be
well sorted out by now – and for the most part,
it is.
The investigation clearly highlighted basic
design flaws and a complete lack of oversight by
every single party that had responsibility to
either identify the design errors or stop work
and call for a safety stand-down, once it was
clear that there was a massive internal failure.
The “what” is very clear but the “why” is more
elusive. Despite the public’s anger, distress,
and disappointment, none of the responsible
organizations had any intent for this tragic
event to occur or to cause any injury or loss of
life. Sadly, good intentions do not suffice for
competence and diligence.
Engineering schools will use this as a landmark
case study for years – and they should.
The Engineer of Record employed by Figg was
experienced, but his calculations were
erroneous. Reflection on this event should go
far beyond merely a technical review. The checks
and balances that were required by the Florida
Department of Transportation (FDOT) and American
Association of State Highway and Transportation
Officials guidance and incumbent upon Louis
Berger, the peer-reviewing organization, were
completely lacking.
Louis Berger lowered its bid to review the
project by 43% in order to get the business, but
also reduced the scope of the review. The reason
given was there wasn’t enough money in the
project to cover its efforts. That’s both
disingenuous and unconscionable. It also was in
violation of FDOT’s requirement that there be an
independent second set of eyes to review
everything – not just what was economically
convenient.
It is likewise incomprehensible and unethical
that Louis Berger would even bid on a job for
which it lacked the requisite qualifications
(see main feature). That FDOT, which was
supposed to review the plans, did not know, or
think to ask, about its qualifications is more
than just an oversight. It’s just plain sloppy.
Ditto for Figg.
FDOT claimed a technical error on the FDOT
website and then, after the collapse, fabricated
a disclaimer that it is not responsible for the
data that it posts. That’s unacceptable in my
view – either ensure the information is accurate
or don’t post it.
The bridge was not properly designed, and there
was no qualified oversight on that design. When
the inevitable began to happen – a creeping,
catastrophic material failure, nobody did
anything, despite what NTSB chairman [Robert]
Sumwalt accurately described as the “bridge
screaming at everyone that it was failing.” Why?
Once the cracking became evident, not one of the
organizations involved was willing to take the
essential and unpopular step to call a halt and
close the road.
This is similar to the circumstances of the
space shuttle Challenger disaster where the
decision was made to launch in extremely cold
weather. The engineers recommended against it
because the O-Rings that were critical to fuel
system integrity would be operating outside
their design parameters. Rationalization,
optimism and schedule pressure contributed to
what has been described in management training
circles as “Group Think.” Strong and confident
personalities persuade everyone that everything
will be OK. Despite misgivings and technical
expertise that advise against such action, the
team moves forward as a group.
It appears that the same mindset was in play
here, in every organization: Figg, Louis Berger,
MCM (the construction company), Bolton Perez
(the engineering firm overseeing the bridge
construction), FDOT, and finally, Florida
International University. It also appears that
every organization absolved themselves of
responsibility by rationalizing that if the
Engineer of Record says it’s OK, it must be OK,
and if anything bad happens – it’s on him. That
is not the intent of peer review or safety
oversight, and certainly fails the system of
checks and balances in place to prevent
catastrophes like these.
The NTSB’s stated role is not to lay blame, but
some would say that’s exactly what we do when we
apportion causation. The human failing that
affects all of us is complacency. It is not a
term the NTSB uses often, but in my opinion, it
is present in nearly every accident and crash.
We are creatures of habit, and when we become
comfortable through long repetitive experience,
the guard often comes down – periodically with
disastrous results. This is precisely what
safety management systems are designed to
prevent – to trap errors in process before they
become catastrophes. While disasters may be
perfectly clear in hindsight, the best
organizations take proactive measures –
constantly.
Schedule pressure, economics, overconfidence,
and complacency all work to counter good
intentions and too often create tragedy.
It is my fervent hope that the organizations
involved will take the NTSB recommendations (see
box) seriously and quickly implement them. The
lives lost and the families disrupted deserve at
least that much.
Key recommendations from the NTSB report
The National Transportation Safety Board made
the following key safety recommendations,
primarily to the Florida Department of
Transportation:
-
Require that the independent peer review for
category 2 bridge structures includes
checking and verifying the design
calculations used for all nodal forces
-
Require
the independent peer-reviewed to submit a
prequalification letter showing that it is
qualified in accordance with Florida
Administrative Code
-
Specify
that when structural cracks are initially
detected during bridge construction, the
engineer of record, construction engineering
inspector, design
and build contractor, or local agency that
owns or is responsible for the bridge
construction immediately close the bridge to
construction personnel and close the road
underneath; fully support the entire bridge
weight using construction techniques that do
not require placing workers on or directly
under the bridge during installation; and
restrict all pedestrian, vehicular, and
construction traffic on the bridge until the
complete support is in place and inspected
-
Require
personnel to monitor and inspect all local
agency bridge projects determined by the
department to have uncommon designs
-
Add
a discussion about redundancy to the
Structures Manual, Structures Design
Guidelines, emphasizing uncommon bridge
designs
Additionally it recommended that the American
Association of State Highway and Transportation
Officials and Federal Highway Administration:
And to Figg:
|


